



Last Monday, the UK’s National Institute for Health and Care Excellence (NICE) held its much anticipated roundtable discussion event, ostensibly to appease those (few) medical stakeholders who had baulked at the newly developed treatment guideline for ME/CFS.
Regular readers will be aware that NICE developed its guideline over several years following a rigorous assessment of the research evidence. However, for reasons that are still a little vague, some senior figures in Britain’s medical establishment let it be known that they were not that comfortable with what had been proposed. Despite the fact that NICE went so far as to pause the publication of its guideline in order to hear them out, the subsequent opportunity for calm discussion at the roundtable threw up no substantive issues. The guideline is now to be published this week, as was intended back in August.
It is, of course, appropriate that medical guidance be shaped by scientific rigour and review. But for years this was far from the case with ME/CFS. The two treatments previously presented as standard care — cognitive behavioural therapy (CBT) and graded exercise therapy (GET) — were each grounded in exceptionally weak science, and appeared to provide little or no benefit to ME/CFS patients. GET, in particular, appeared to be worse than merely useless; in many cases, it has been shown to damage patients’ well-being.
The recent history of the field has not reflected well on British medicine or, by extension, British psychology. Perhaps understandably hamstrung by cognitive dissonance, a number of senior academic panjandrums spent years sticking gamely to their guns, insisting that the therapies that they themselves developed, and drawn from medical theories that they themselves formulated, simply must be of value, no matter what the scientific data had to say.
* * *
In an ideal world, scientific evidence would have won out long ago. But the world we live in is far from ideal. And so it came to pass that these iffy therapies were dished out to thousands of patients, essentially on the say-so of so-called senior experts.
Like zealous internet conspiracy theorists, these folks insisted they had “done their own research.” They used this work to convince themselves, and their like-minded acolytes, that all was well.
However, when NICE conducted a formal evidence review as part of the development process for its new treatment guideline, it found that all the studies (not just most of them, but literally all of them) were so weakly designed as to produce evidence that was uniformly of “low” or “very low” quality. As evidence reviews go, it was quite the bloodbath.
The chief deficiency in any study on CBT and GET for ME/CFS is nearly always the same: an over-reliance on self-report measures in what are inevitably unblinded trials. Other frequent flaws include the ignoring of participant selection biases and study dropout rates, and an unflattering habit of re-prioritising study aims after-the-fact. In academic studies of psychology’s replication crisis, these well-acknowledged scientific problems have become recognised red flags. They are commonly referred to as QRPs, or Questionable Research Practices.
Of course, the studies in question had been published in medical journals, implying that each had been passed through a process of peer-review. Many were also approved by agencies that provided research funding. The fact that they were all eventually exposed as being substandard is just the latest demonstration of how modern academia’s supposed ‘quality control’ systems are plagued by critical shortcomings.
In reality, this community of clinicians had cultivated their own academic echo chamber. Their bad studies were indeed subjected to review processes, but the reviewers were mostly other investigators who themselves were conducting similarly bad research. This is one of the reasons why all these studies were based on variations of the same design, and why all were lumbered with the same methodological flaws.
When a tight-knit network of researchers ends up reviewing one another’s trials, assessment of quality cannot be truly independent. Peer-review, as it was originally intended, ceases to function.
The new NICE review was essentially an exposé of bad science. It lifted the rock on this branch of research and revealed the ugly truth of what wriggled underneath.
* * *
Perhaps it is no surprise that the researchers whose work was most maligned immediately went into a panic, choosing to lash out at the NICE process itself. It is equally unsurprising that when given the opportunity, they could offer no argument with which to defend themselves.
In short, the evidence simply doesn’t support the use of either CBT or GET as ME/CFS treatments. NICE will publish its new guideline to this effect in the coming days.
But cognitive dissonance is a powerful force, and we can fully expect continued denials from the conspiratorial fringe. Already a new academic paper has appeared. It was written and reviewed before NICE’s new guideline was published (and before its roundtable meeting), but presumably after the authors had seen NICE’s evidence review, which appeared last November.
The symptoms of denialism are vividly apparent in the language of this new publication. The authors write as if NICE said nothing about the quality of previous research. Within the abstract alone, this denialism is signposted in at least two ways.
Firstly, the paper baldly states the following:
The main evidence-based treatments are rehabilitative in nature and include specific types of cognitive behavior therapy (CBT), and graded exercise therapy (GET).
But obviously NICE has shown that these two therapies are not evidence-based at all. Simply saying so in a new paper does not alter this reality. In fact, making this claim in the full knowledge of what NICE has found suggests little more than a contempt for NICE’s role in the regulation of medical standards, as well as a disregard for the general principle of independent scientific review.
Secondly, the authors refer to these conditions as “CFS/ME” and not “ME/CFS”. Patients and dispassionate researchers will immediately recognise the significance of this choice of language. Placing “CFS” ahead of “ME” implies that these illnesses are chiefly characterised by “chronic fatigue” symptoms, rather than by the neurological dysfunction encapsulated in the term myalgic encephalomyelitis.
Privileging “CFS” is the authors’ subtle way of foregrounding their preferred worldview — that the symptoms these patients experience are psychogenic in nature and so are legitimately curable using CBT and GET.
(And while patient groups caution against combining the labels “ME” and “CFS” into a single title, when forced to choose, they invariably opt for “ME/CFS” over the alternative order. The authors of this new paper will have been well aware of that preference.)
The authors suggest that they use “CFS/ME” because this is a term that is used “often”. But just as they stretch the meaning of “evidence-based” to its elastic limit, their interpretation of the term “often” also seems quite ductile.
Take a look at the Google search results for “CFS/ME” compared to those for “ME/CFS”:
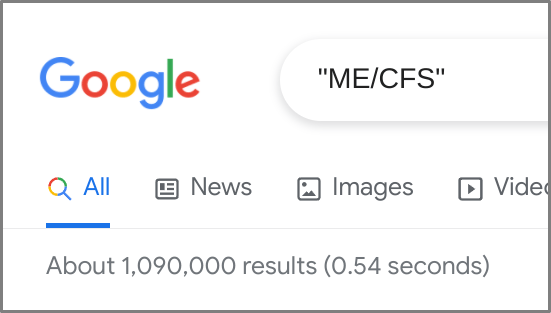
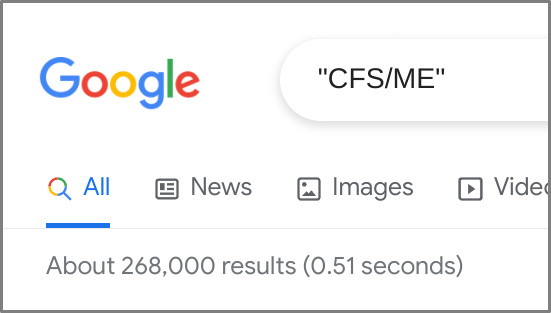
“ME/CFS” returns over a million search results, whereas “CFS/ME” returns just 268,000. In other words, “ME/CFS” is clearly the more common term; “CFS/ME” is, relatively speaking, the less obvious choice.
The dog-whistling here will be familiar to patient advocates and other observers of this field. Whenever “CFS/ME” appears in print, it is a sure sign that its authors are going out of their way to make a dogmatically arbitrary point.
* * *
The new NICE guideline for ME/CFS represents a refreshingly welcome change. By contrast, the continuing denials of those clinicians still wedded to what are demonstrably obsolete treatment practices are, unfortunately, never going to go away.
They will continue to refer to their remedies as “evidence-based” when they are clearly not, and they will go on calling these illnesses “CFS/ME” instead of “ME/CFS” because that’s what suits their agenda.
Perhaps they feel that by repeating these things over and over, they can brainwash us all into internalising their denialist worldview.
Maybe they feel they can persuade us that these illnesses are rooted in psychological processes and are thus amenable to psychological and behavioural treatment. Maybe they think they can get us to believe that ME/CFS patients are engaged in a self-destructive pattern of unhelpful cognitions, malingering, and deconditioning. Maybe they think they can finally convince us that ME/CFS is a souped-up personality problem preventing patients from comprehending that there is nothing actually wrong with their bodies. If they just keep saying it, maybe we’ll all start believing it…
Whatcha gonna do? Gaslighters gonna gaslight.
As ever in life, some things change, some stay the same. There will always be those who will never accept that things are different now, but these people’s positions are fatally untenable and their influence will slowly wane.
Out here in the real world, we move on.

Brian Hughes is an academic psychologist and university professor in Galway, Ireland, specialising in stress, health, and the application of psychology to social issues. He writes widely on the psychology of empiricism and of empirically disputable claims, especially as they pertain to science, health, medicine, and politics.
Pingback: Reactions to NICE having “paused” the release of the revised Guideline on ME/CFS | On Eagles Wings
Pingback: Facebook Group activity in October - DGMEFM Network