



Swiss Re Group, “one of the world’s leading providers of reinsurance and insurance,” recently hosted a virtual Expert Forum on “secondary” impacts of COVID. As would be expected, the insurance industry is especially interested in the financial implications of this new disease. The programme covered many of the biophysical sequelae of COVID, as well as its knock-on impact on population mental health and the effects of lockdown-related treatment delays. Many of the slide presentations are now online.
What with all that lung fibrosis, myocardial injury, kidney damage, and hair loss — not forgetting those purple toes — the long term impacts of COVID will have the insurance industry busy re-computing its premiums for quite some time to come. It’s a for-profit business, after all.
Of course, you can’t have a gravy train without folks trying to hop aboard.
And it looks like at least one of the Swiss Re speakers was in a dash to switch tracks.
* * *
As extensively covered in this blog, the UK gravy train directing thousands of British ME/CFS patients to meritless psychological therapies has recently begun to slow down — after NICE published new draft treatment guidlines rejecting such practices as CBT, GET, and the so-called “Lightning Process.” It is set to grind to a complete halt next August.
But just as the ME/CFS gravy train begins to apply its brakes, lo and behold, the Long COVID Express pulls into the station. Choo choo!
Simply put, the people who for years have been presenting CBT and GET as ME/CFS treatments are now pitching their wares at the Long COVID community. Already they have been applying the same hysteria-based schtick. Long COVID, they claim, is in most cases propelled by psychological factors (a euphemistic way of saying that it’s all in the mind). You can even cure it with positive thinking.
If, say, you are an insurance company, you need not worry about costly medical bills. These folks are ready to testify that CBT and GET will do the job just fine.
It’s a win-win situation: the insurance industry gets to pay out minimal fees for time-limited talk therapies, while the talk therapists get to continue to provide their treatments to the world.
* * *
Among the speakers at the Swiss Re event was none other than a co-author of the much beleaguered PACE Trial, one of the most expensive studies of psychobehavioural interventions ever conducted in the UK — and, in terms of its flaws, possibly one of the weakest. The NICE reviewers found the overall evidence base provided by PACE (and similar studies) to be of uniformly “low quality”.
But the PACE Trial emanated from an esteemed British university, and was published in an esteemed journal. So there. Eminence-based medicine and all that.
This person’s slides make for interesting reading — that is to say, if, like me, you are interested in confirmation bias among scientists, the exaggeration crisis in psychology, the reasons why research studies fail, and the way clinical myths become perpetuated.
In other words, they are well worth a look.
* * *
Here, for example, is an opening snippet, part of the scene-setting section of the presentation:

I guess what jumped out most for me from this slide is that bullet point referring to “Females”. You see, the people who want you to believe that confusing physical illnesses are “all in the mind” have been adopting a cherchez-la-femme approach for years. They are fascinated by conditions that appear more commonly in women than in men. The very fact that women get these illnesses is considered de facto evidence of mass hysteria. Medics might not be explicit using that argument any more, but the problem of embedded sexism in healthcare has a long and consistent history.
I recently wrote about how this very reasoning was used by the authors of the 1970 BMJ paper that launched the entire psychogenic approach to ME. George Monbiot was kind enough to cite my post in his widely lauded Guardian piece on Long COVID. We will come back to George below.
* * *
Here is another slide. It features a woman:

You can take it that those items marked in red are intended to highlight the speaker’s argument that Long COVID symptoms are mostly self-reported. This in turn is linked to the theory that they are not real symptoms (hashtag I-don’t-believe-her).
The citation on the slide is to this item in JAMA from last August. The item is not quite a research article, but an extended letter to the editor submitted by a group of medics from Italy. They used it to report the characteristics of 143 COVID patients, the majority of whom continued to report symptoms long after they were discharged from hospital. All patients who met the study criteria during a one-month period were invited to participate.
Sixty-three per cent of the sample were men, far removed from the sweeping generalisation on the previous slide that it is “Females” who get Long COVID.
Also, the JAMA letter did not use that diagram of Long COVID Woman. It looks like the PACE Trial author might have mocked it up himself.
* * *
The presentation goes full tilt on the psychogenic hysteria theory. There are several slides arguing that much (if not most) Long COVID is rooted in mass anxiety, provoked by fantastical media coverage and reckless patient-group advocacy.
Here’s George Monbiot again, contributing to mass hysteria with his pesky factual claims — many of which, incidentally, were the very same points made by other speakers at the Swiss Re event:

And these support groups, what are they thinking offering all that support? Shame on them:
I guess many of us will be reminded of another PACE acolyte who once expressed the view that his “spirits sink” every time we have events such as “mental health awareness week”. These folks have long believed that ordinary people just cannot be trusted to think about illness without becoming convinced they are seriously sick.
Here is the slide that summarises all the “possible causes” of Long COVID. Note how the vast majority of them are psychological, behavioural, or social:
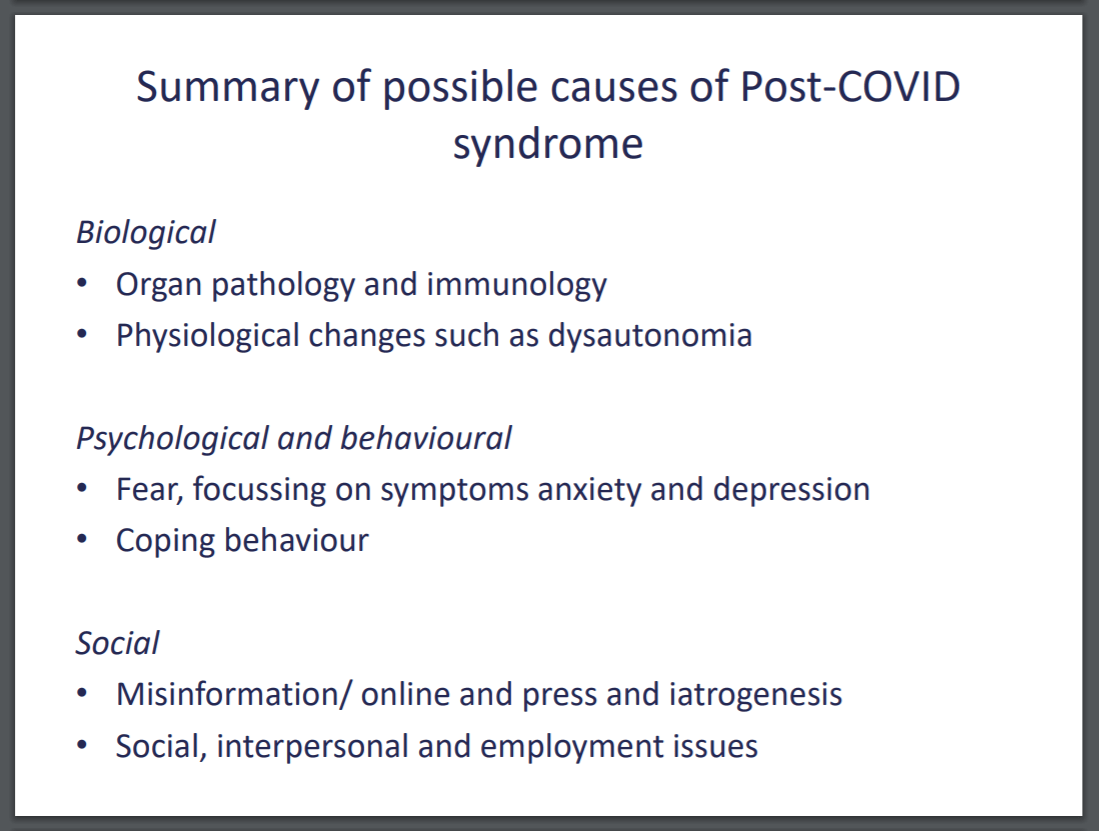
All the better with which to be treated using CBT, I suppose.
(By the way, for readers not in the know, in this context “employment issues” is a reference to malingering — because, as the psychogenic theory goes, many of those hysterical patients are really just trying to get off work.)
* * *
And then there were the case studies. Because nothing says “Beware of misleading socially shared beliefs” better than a couple of hand-picked case studies.
The first was from the speaker’s own clinic. One hundred per cent of this person was female:

Three small children, eh? Nothing gendered about this at all. Unfortunately the woman was unable to work.
However, the man in the second case study was not only able to work, he was able to cure himself of Long COVID by the power of positive thinking:
I don’t know how many children this guy has, but we are informed of the critical detail that he is a professor of medicine.
Of course, as I have written previously, the fact that this man recovered from Long COVID is neither here nor there. His status as a one-person-sample sheds light on nothing. And despite the title of the slide, this man’s experience was not written up as a “Case Study” in the esteemed BMJ. It was basically his personal diary as recorded in his regular op-ed column. In other words, he wrote it himself.
The BMJ has strict guidelines for writing case reports. This autobiographical reflection should not really be framed as a medical journal “case study”.
* * *
The speaker spent a few slides relitigating the now-doomed PACE Trial, as well as criticising those who have suggested that ME is a physical illness and so unlikely to be treatable using psychological therapy. He doesn’t appear to mention that this latter group includes such jumped up non-entities as the World Health Organization and the US National Academy of Medicine.
And here is what the speaker feels is the likely outcome of Long COVID. See if you can spot any assertions that are supported by evidence (spoiler alert — there aren’t any):

The final summary slide included this gloriously evidence-free claim: “At present the best treatment [for Long COVID] is psychologically informed rehabilitation.” The phrase “at present” is doing a lot of heavy lifting there.
Of course, it would be ethically complicated for a clinician who provides a particular service to promote that very same service when speaking to a financial paymaster. So, while not discernible from his PowerPoint, I am sure the speaker must have ended his presentation with a verbal disclaimer warning his audience to bear in mind his conflict of interest, and to take everything he just said with a pinch of salt…
The slides can be downloaded from the Swiss Re website here. Get them while you still can.
Choo choo!


Brian Hughes is an academic psychologist and university professor in Galway, Ireland, specialising in stress, health, and the application of psychology to social issues. He writes widely on the psychology of empiricism and of empirically disputable claims, especially as they pertain to science, health, medicine, and politics.
